In its simplest definition, Interventional Cardiology is a subspecialty that deals specifically with catheter-based treatment of heart diseases. Catheterization is a procedure that involves the insertion of a sheath into the groin or wrist artery and passing a catheter to the heart. Common procedures performed by SDCA interventionalists by catheterization are, Angioplasty, Stent, Atherectomy, Patent Foramen Ovale (PFO) closure, Left Atrial Appendage Occlusion, Transcatheter Aortic Valve Replacement TAVR, and MitraClip.
In this video, Interventional Cardiologist Jeb Burchenal discusses the symptoms of a heart attack and the importance of calling 911. He also talks about coronary intervention and stopping a heart attack with a stent through coronary catheterization.
These procedures may be performed immediately after the catheterization or at a later time, depending on the circumstances. If you have any of the following procedures, they usually last an additional 1-2 hours beyond the catheterization procedure. You will spend the night at the hospital and be able to return home the next morning.

Balloon angioplasty (percutaneous transluminal coronary angioplasty or PTCA)
This is performed by inserting a specially designed catheter with a small balloon tip into the narrowed coronary artery. Once the catheter is in place, the balloon is inflated to compress the plaque (fat deposit) into the artery wall, increasing blood flow to the heart. When the balloon is inflated at the point of the blockage, you may feel chest pressure or discomfort, which is normal. It will subside when the balloon is deflated. You may also feel your heart thump or skip, feel flushed, or have a headache. All of these sensations are normal. The success rate of this procedure by itself is 70-80%, and people will have diminished chest pain and reduce their risk for heart attack. Approximately 20-30% of those undergoing PTCA will have re-narrow the artery (restenosis) and need a repeat PTCA or a stent within 3-12 months. The risks of this procedure are similar to cardiac catheterization; however, there is an added risk of abrupt closure of the artery, which may result in a heart attack or require emergency coronary artery bypass surgery. In rare instances, the artery can separate from the wall (dissection), requiring emergency surgery as well.
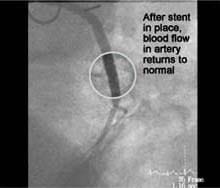
Stent
A stent is a tiny tube made out of stainless steel. It looks similar to the “Chinese handcuffs” you might have played with as a child and is used as a scaffolding to keep the artery open. It is often used with PTCA to decrease the risk of the artery re-narrowing. After opening the vessel, the stent is placed with a different catheter that places the stent and then expands the stent with a balloon. The balloon and catheter are then removed. The stent stays in place permanently, and over the next several weeks, the artery actually “heals” around the stent.
Atherectomy
For this special procedure, a special catheter with a special tip is guided to the point of narrowing in the coronary artery. The tip will either grind or shave the plaque. Depending on the procedure, the shavings will be “caught” in a special chamber in the catheter and removed, or if ground, the microscopic particles are washed safely away in the bloodstream.
Patent Foramen Ovale (PFO) Closure
PFO is a small opening between the two upper chambers of the heart that did not close at birth, A small, flexible tube (catheter) into an artery in the groin and threaded through the blood vessel all the way to the PFO. This tube will have a small device inside it. This device will be inserted between the abnormal opening between the upper chambers and deployed, which occludes the abnormal hole. After a time, the inside lining of the heart will grow over the device. Our Structural Heart Clinic will follow these patients.
Left Atrial Appendage Occlusion
Stroke is a serious risk for those who have Atrial Fibrillation because of the chance of forming blood clots in the heart and setting them free to the brain. Most clots are believed to come from the Left Atrial Appendage (LAA) in the heart’s left atrium, which is something like an appendix in the abdomen. This LAA has no specific function and is not needed for heart function. Instead of removing the appendage like the appendix, it is occluded with a small device called the WATCHMAN Implant. The procedure consists of advancing a catheter through the leg and the bloodstream until it reaches the heart’s upper right chamber. The cardiologist will make a small hole through the wall between the two upper chambers of the heart so that the catheter reaches the left atrium. The cardiologist then pushes the device through the delivery catheter into the left atrial appendage, where it opens up like an umbrella and is permanently implanted. Once the device is in place, a thin layer of tissue grows over it in about a month and a half. Our Structural Heart Clinic follows these patients.
Transcatheter Aortic Valve Replacement (TAVR)
Transcatheter Aortic Valve Replacement (TAVR) is a procedure performed through a catheter inserted into the patient’s groin, which provides treatment for patients with aortic stenosis considered too high of a risk for open-heart surgery. The procedure is similar to a cardiac stent. Instead, a stent-like device is deployed across the aortic valve creating a wider opening. TAVR received FDA approval in the fall of 2011. These patients are followed by our Structural Heart Clinic.
MitraClip
Mitral regurgitation is the most common heart valve disorder in the United States. Mitral regurgitation is a condition when the leaflets of the valve do not close properly, and blood flows backward into the upper chamber. Over time, this condition can create symptoms and produce abnormal heart rhythms, clots, or, in many cases, heart failure. The usual treatment for mitral regurgitation is open-heart surgery to repair or replace the leaky valve. However, surgery is not for everyone. When open-heart surgery is too risky, the MitraClip device may be a good alternative. During this procedure, physicians thread a catheter from the leg to the heart and place a MitraClip device to decrease blood backflow. This clip allows the mitral valve to close more completely, helping to restore normal blood flow to the heart. Often, many times patients go home the next day. Our Structural Heart Clinic follows these patients.
After all of these procedures, there are specific instructions your cardiologist will want you to follow. Upon discharge from the hospital, a patient discharge booklet will be given to you will all the instructions you will need for your aftercare.
 Cinthia Bateman, MD
Cinthia Bateman, MD Jeb Burchenal, MD
Jeb Burchenal, MD Anthony J Cedrone, MD
Anthony J Cedrone, MD Ira Dauber, MD
Ira Dauber, MD Sean A. Enkiri, MD
Sean A. Enkiri, MD Dimitri Kaufman, MD
Dimitri Kaufman, MD Lee MacDonald, MD
Lee MacDonald, MD Erin Unger, MD
Erin Unger, MD